What is Musculoskeletal and Joint Pain?
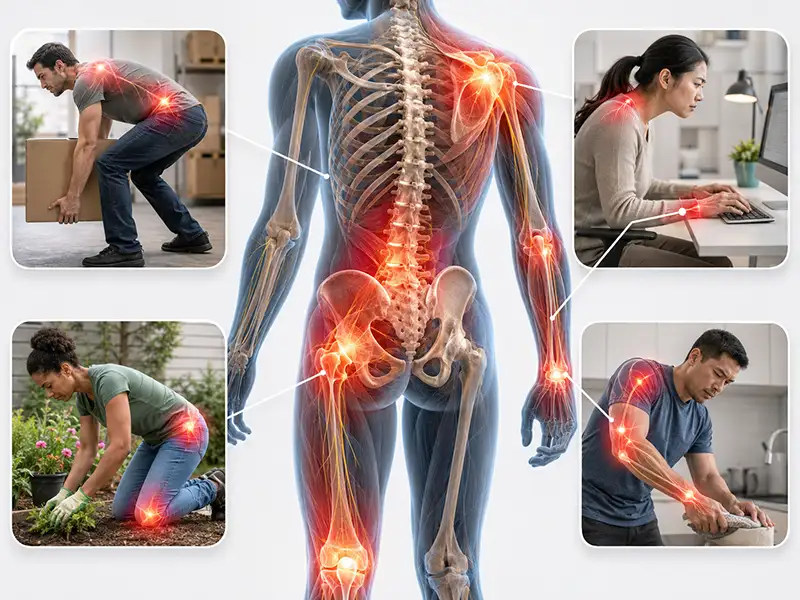
Musculoskeletal and joint pain shows up differently for everyone. For some, it is a nagging ache in the knee that flares after a long walk. For others, the stiffness is so severe in the morning that getting out of bed takes real effort. What these experiences share is an origin somewhere within the body’s structural system: bones, muscles, cartilage, tendons, ligaments, or the joints where these components meet.
The musculoskeletal system works as a coordinated network. Bones provide structure, muscles generate movement, tendons anchor muscles to bone, ligaments stabilize joints, and cartilage cushions the surfaces where bones meet. When any part of that system is disrupted, whether by injury, wear, inflammation, or disease, pain and reduced function tend to follow.
One thing that surprises many people is how interconnected these structures are. A knee problem can quietly alter the way you walk, which over time places excess stress on the hip or lower back. By the time the secondary pain becomes the primary complaint, the original problem has sometimes been overlooked for months. Getting a clear, accurate diagnosis early makes a meaningful difference in how well treatment works and how fully function can be restored. If musculoskeletal or joint pain is affecting your daily life, Shore Spine & Pain offers the diagnostic expertise and targeted treatment options to identify the source and address it directly.
What Causes Musculoskeletal and Joint Pain?
Pain in the muscles and joints rarely has a single cause. Age, prior injuries, activity level, body weight, and genetics all play a role, and in many cases more than one factor is at work simultaneously.
- Degenerative Conditions: Osteoarthritis is the most common culprit, particularly in adults over 50. As cartilage wears down, bones begin making contact during movement, generating friction, swelling, and pain that worsens over time. The knees, hips, hands, and spine are affected most often. In the spine, this process is closely related to degenerative disc disease and facet joint syndrome, 2 of the most common drivers of chronic spinal pain.
- Inflammatory Conditions: Rheumatoid arthritis is an autoimmune disease in which the immune system attacks the joint lining, causing persistent swelling, warmth, and pain that typically affects both sides of the body. Bursitis and tendinitis are more localized forms of inflammation near a joint rather than within it, commonly occurring around the shoulder, elbow, hip, and knee.
- Acute Injuries: Ligament sprains, muscle strains, stress fractures, rotator cuff tears, and cartilage damage can all produce significant joint pain. What often goes underappreciated is how much unresolved acute injury contributes to chronic pain years later, as even a minor sprain that was walked off without proper care can leave a joint subtly unstable and more vulnerable to early arthritis.
- Overuse and Postural Strain: Repetitive motions accumulate load on specific joints and tissues over time, and when that load exceeds the body’s capacity to recover, pain and reduced function follow. Poor posture, prolonged desk work, and non-neutral body mechanics place similar cumulative demands on the spine, hips, and knees, often without any single identifiable moment of injury.
- Systemic and Metabolic Factors: Gout produces sudden, intensely painful joint flares from uric acid crystal buildup, most commonly in the big toe, ankle, or knee. Fibromyalgia causes widespread musculoskeletal pain alongside fatigue and disrupted sleep. Vitamin D deficiency and excess body weight each contribute independently, the former by weakening bone and muscle, the latter by accelerating cartilage breakdown and promoting low-grade systemic inflammation.
Symptoms of Musculoskeletal and Joint Pain
Symptoms range from a dull, predictable ache to sharp pain that appears without warning. Some notice a gradual change in what they can do, finding over months that stairs have become harder or that reaching overhead now requires conscious thought. Others experience a sudden onset with a clear triggering event.
- Pain: The most consistent complaint, presenting in many ways. It may be present at rest, brought on by specific movements, or felt only when bearing weight on a limb. The character of the pain, whether burning, stabbing, throbbing, or aching, often provides useful diagnostic information.
- Stiffness: Following sleep or a period of sitting is a common early sign of joint disease. In inflammatory conditions, morning stiffness tends to last longer and ease only gradually with movement. In osteoarthritis, it typically resolves more quickly once the joint warms up.
- Swelling, Redness, and Warmth: Signal active inflammation and warrant prompt evaluation, as they can indicate anything from a flare of chronic arthritis to an acute injury or, less commonly, a joint infection.
- Reduced Range of Motion: Affects quality of life in ways that are easy to normalize before seeking care. Difficulty turning the neck to check a blind spot, struggling to squat, or losing the ability to fully straighten a knee are all signs that structural changes within the joint deserve attention. This can overlap with conditions such as spinal stenosis and sacroiliac joint pain, making accurate diagnosis an essential first step.
- Muscle Weakness and Fatigue: Near an affected joint can develop both as a direct effect of the underlying condition and as a consequence of reduced activity over time. Weakness around a joint reduces its stability, which often creates a feedback loop that accelerates the underlying problem.
- Mechanical Symptoms: Such as grinding, clicking, popping, or a locking sensation during movement typically reflect structural changes inside the joint, including cartilage loss, loose bodies, or meniscal damage.
The longer musculoskeletal and joint pain goes unaddressed, the more of your daily life it tends to claim. Shore Spine & Pain in Lakewood, NJ and Shrewsbury, NJ is ready to help you stop that pattern.
Treatments We Offer for Musculoskeletal and Joint Pain

Musculoskeletal and joint pain responds best to treatment that is matched to its cause and calibrated to your goals.
Interventional Pain Management:
- Facet Joint Injections: When arthritic or inflamed joints are the primary source of pain, a corticosteroid delivered directly into the affected joint reduces inflammation and provides targeted relief, with effects that can last weeks to months depending on the underlying condition.
- Radiofrequency Ablation: For confirmed joint-mediated pain, radiofrequency ablation uses precisely directed heat energy to interrupt the nerve signals transmitting pain from the affected joint, offering relief that extends considerably beyond what injection therapy alone can provide.
- SI Joint Injection: For pain originating at the sacroiliac joint, a targeted injection confirms the diagnosis and delivers direct anti-inflammatory relief, serving both a therapeutic and a diagnostic function.
- Spinal Cord Stimulation: For musculoskeletal pain that has become chronic and complex, particularly when a significant nerve component is present, spinal cord stimulation modifies how pain signals travel through the nervous system before they reach the brain. Rather than targeting the joint or tissue directly, it addresses the way pain is perceived, often providing meaningful relief for those who have not responded to conventional approaches.
- Peripheral Nerve Stimulation: In select cases where pain is localized along a specific nerve pathway, peripheral nerve stimulation delivers targeted neuromodulation directly where it is needed, offering a complementary option alongside spinal cord stimulation for chronic nerve-driven joint pain.
Chronic joint and musculoskeletal pain has a way of narrowing what feels possible. At Shore Spine & Pain, Dr. Woska works with you to change that, building a joint pain treatment plan based on a precise understanding of your condition and a clear commitment to getting you back to the pain-free life you deserve.
Frequently Asked Questions about Musculoskeletal and Joint Pain
How do I know if my joint pain requires medical attention or if it will resolve on its own?
Pain that lasts more than a few weeks, limits your ability to perform normal daily activities, or is accompanied by swelling, warmth, or significant stiffness warrants an evaluation. Acute pain from a minor strain will often settle with rest and over-the-counter medication within a week or two. When it does not, or when symptoms come and go but keep returning, there is usually something worth investigating.
Does joint pain always mean arthritis?
Not necessarily. Arthritis is one of the more common causes of persistent joint pain, but bursitis, tendinopathy, ligament damage, nerve-referred pain, and structural instability can each produce similar symptoms without involving cartilage breakdown. This is one of the reasons an accurate diagnosis matters before treatment begins, because the distinction between these causes directly determines which treatment is most likely to work.
Can musculoskeletal and joint pain affect people of all ages?
Yes. While degenerative conditions like osteoarthritis are more prevalent in older adults, musculoskeletal pain from overuse injuries, sports-related damage, and inflammatory conditions is common at every age.
I have been told I have arthritis, but my pain seems to be getting worse. Is that normal?
Arthritis is a progressive condition, meaning the underlying joint changes tend to advance over time, particularly without treatment or management. That said, increasing pain is not something to simply accept as inevitable. Changes in activity level, body weight, inflammation, or the development of a secondary problem in an adjacent joint can all contribute to worsening symptoms. A re-evaluation at Shore Spine & Pain in Lakewood or Shrewsbury, NJ can help determine whether the progression is expected or whether something new is contributing to the change.
Will I need surgery for my joint pain?
Most cases of musculoskeletal and joint pain do not require surgery, at least not as a first step. Surgery becomes a genuine consideration when structural damage is severe, when non-surgical options have been tried thoroughly and fallen short, or when functional goals cannot realistically be met any other way.