What is a Vertebral Compression Fracture?
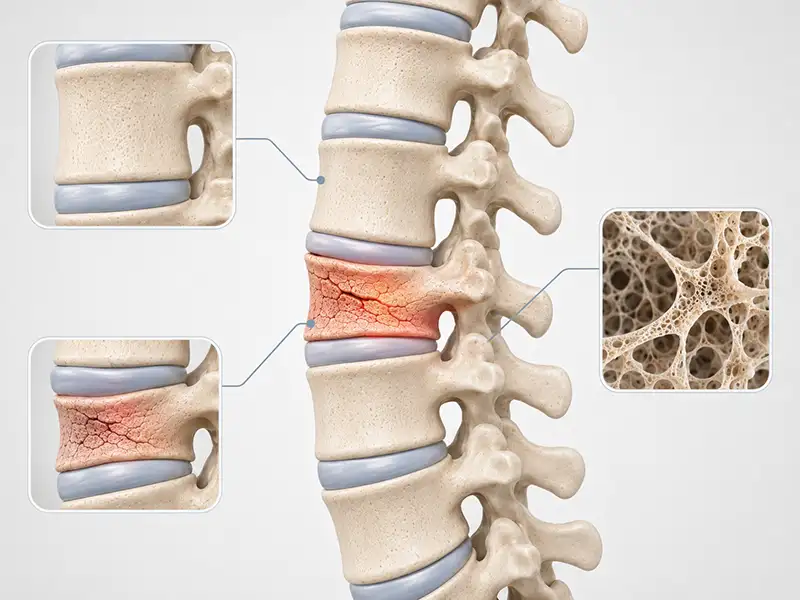
A vertebral compression fracture occurs when a vertebra cracks or partially collapses under pressure, and it loses height and takes on a wedge-like shape. That structural change can gradually alter the natural curve of the spine, sometimes leading to a rounded or hunched posture that is often noticeable before a diagnosis has been made.
These fractures most commonly affect the thoracic spine (mid-back) and the upper lumbar spine (lower back), regions that absorb a disproportionate share of the body’s load throughout the day. Many go undetected for months because the pain is easy to dismiss as ordinary back stiffness.
If you are experiencing sudden or worsening back pain in the Lakewood or Shrewsbury, NJ area, particularly with a history of osteoporosis or prior spinal injury, Shore Spine & Pain offers the diagnostic expertise and minimally invasive treatment options to identify the source and address it directly.
What Causes a Vertebral Compression Fracture?

Vertebral compression fractures can develop for several different reasons, and understanding the cause is an important part of finding the right treatment. Common causes of a vertebral compression fracture includes:
- Osteoporosis: This is the most common cause. As bones lose density over time, the vertebrae become more fragile and easier to fracture. In advanced osteoporosis, a vertebra can fracture during something as minor as a sneeze, a cough, or reaching for an object on a low shelf. This connection between degenerative disc disease and declining spinal structure is why early evaluation matters for anyone with known bone density loss.
- Trauma: In younger or otherwise healthy people, compression fractures are usually the result of a significant impact. A hard fall, a car accident, or a high-impact sports injury can place enough sudden force on the spine to fracture even a healthy vertebra.
- Cancer and Metastatic Disease: Tumors that spread to spinal bone from the breast, lung, prostate, or kidneys, as well as multiple myeloma, a blood cancer that attacks bone marrow directly, can weaken a vertebra from within until it gives way. This is an important diagnostic consideration when a fracture occurs without clear mechanical cause.
- Long-Term Corticosteroid Use: Extended use of corticosteroid medications suppresses the processes the body relies on to maintain bone density, increasing fracture risk over time even in the absence of other risk factors.
Symptoms of a Vertebral Compression Fracture
Not every vertebral compression fracture announces itself with dramatic, immediate pain. Fractures caused by osteoporosis in particular can develop gradually and silently, with some discovered only when imaging is ordered for an unrelated reason.
When symptoms are present, the most common is a deep, localized ache in the mid or lower back that gets worse with standing, walking, or twisting and feels noticeably better when lying down. This pattern, pain that eases at rest and worsens with activity, is one of the more telling signs that a fracture rather than a muscle strain may be responsible.
When multiple fractures occur over time, measurable height loss becomes common. The spine can develop an exaggerated forward curve, sometimes called a dowager’s hump, that shifts your posture forward and places ongoing strain on the surrounding muscles. Many people also notice fatigue from the effort of staying upright, and in some cases limited ability to take a full deep breath.
In more serious cases, a fracture can put pressure on nearby nerves, producing pain, numbness, tingling, or weakness that radiates into the arms or legs depending on where in the spine the fracture has occurred. If you are experiencing any of these symptoms, the team at Shore Spine & Pain is here to help you find answers.
Treatments We Offer for Vertebral Compression Fracture
A vertebral compression fracture can range from a manageable source of back pain to a significant disruption of daily function, and the right approach depends entirely on the specifics of your situation. At Shore Spine & Pain in Lakewood, NJ and Shrewsbury, NJ, Dr. Woska takes the time to understand what caused the fracture, how it is affecting you, and what combination of treatments gives you the best path to recovery.
Interventional Options:
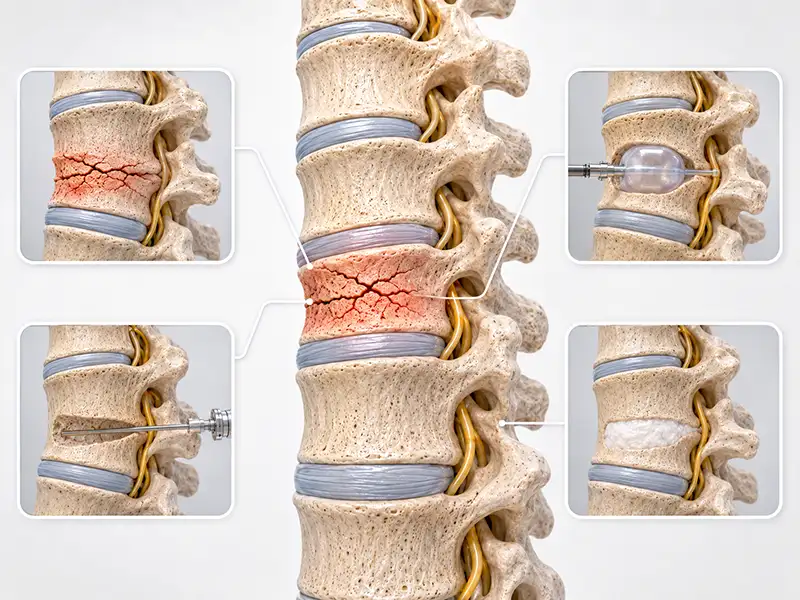
- Kyphoplasty/Vertebroplasty: When conservative care does not provide adequate relief, kyphoplasty is among the most effective minimally invasive options available for vertebral compression fractures. A small balloon is carefully inserted into the collapsed vertebra and inflated to help restore lost height and create an internal cavity. Once removed, bone cement is injected into that space, where it hardens quickly to stabilize the fracture from within. Many people experience meaningful pain relief within days of the procedure, with a relatively short recovery period and no general anesthesia required.
- Spinal Cord Stimulation: For those who continue to experience chronic nerve pain following a fracture, even after the fracture itself has been stabilized, spinal cord stimulation offers a long-term option by modulating pain signals before they reach the brain.
- Peripheral Nerve Stimulation: In select cases where pain remains localized along a specific nerve pathway following fracture treatment, peripheral nerve stimulation delivers targeted relief directly where it is needed.
Recovery from a vertebral compression fracture looks different for everyone, and your care should reflect that. Dr. Woska works with you from initial evaluation through treatment and beyond, to ensure your plan stays aligned with your progress and your goals.
Frequently Asked Questions about a Vertebral Compression Fracture
How do I know if my back pain is a compression fracture
or just a muscle strain?
Muscle strains typically respond to rest, heat, and over-the-counter pain relief within a few days. A vertebral compression fracture tends to produce deeper, more localized pain that is tied closely to position, worse when upright and better when lying flat, and does not follow the usual pattern of a soft tissue injury. Sudden onset pain in the mid or lower back, particularly in someone over 50 or with a history of osteoporosis, is worth investigating with imaging rather than waiting out.
Can a vertebral compression fracture heal on its own?
Some can, particularly when the fracture is minor and the surrounding bone is otherwise healthy. With adequate rest, bracing, and time, the vertebra may stabilize over a period of several weeks to a few months. The concern with osteoporosis-related fractures is that the bone is already compromised, so healing is slower and incomplete, and the altered shape of the vertebra often remains even after pain subsides. Untreated fractures also raise the likelihood of additional fractures nearby.
Will I lose height permanently after a compression fracture?
Height loss depends on how many vertebrae are affected, how much each one has collapsed, and how quickly treatment is initiated. A single fracture treated promptly may result in minimal permanent change. Multiple fractures that go unaddressed for an extended period tend to produce more noticeable and lasting height reduction.
Can a vertebral compression fracture lead to additional fractures in the future?
Yes, and it is one of the more consequential aspects of fracture management that is easy to overlook once immediate pain is addressed. A single compression fracture meaningfully increases the risk of subsequent fractures, both at adjacent vertebral levels now absorbing redistributed load and throughout the spine if the underlying cause of bone fragility is not addressed. This is one of the reasons Dr. Woska approaches vertebral compression fractures with the full clinical picture in mind, because treating the fracture alone without addressing what allowed it to occur leaves the spine vulnerable to the same problem again.
Are compression fractures more common in women?
Yes, significantly so. Women lose bone density at a faster rate after menopause due to the drop in estrogen, which plays a protective role in bone maintenance. That said, men are not exempt, particularly those with a history of long-term corticosteroid use, heavy alcohol consumption, or low testosterone.